AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8965/088
1Assistant professor of Obstetrics and Gynecology, Faculty of Medicine. Tanta University, Tanta. Egypt.
2Lecturer of Diagnostic Radiology, Diagnostic Radiology Department. Faculty of Medicine. Tanta University, Tanta. Egypt.
*Corresponding Author: Naglaa Ali Mohammed Hussein, Assistant Professor of Obstetrics and Gynecology, Faculty of Medicine. Tanta University, Tanta. Egypt.
Citation: Naglaa A. M. Hussein, Mohammed H. E. Refaey, (2021) Evaluation of sonographic measurement of umbilical cord coiling index in the second trimester and its correlation to perinatal outcome J.Obstetrics Gynecology and Reproductive Sciences 5(5) DOI:10.31579/2578-8965/088
Copyright: © 2021, Naglaa Ali M. Hussein, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 July 2021 | Accepted: 15 July 2021 | Published: 09 August 2021
Keywords: umbilical cord; intrauterine fetal death; hypo- and hyper-coiling
Abstract
The umbilical cord represents a unique lifeline between the fetus andmother and contains two arteries and one vein wrapped up in Wharton’s jelly with moderate twists. Umbilical coiling abnormalities canresult in fetal growth restriction, fetal distress, or intrauterine fetal death.
Hypocoiled umbilical cords are associated with intrauterine fetal death (IUFD), fetal growth restriction, fetal distress, low Apgar scores, fetal congenital anomalies, and abnormal insertion of the umbilical cord. Hypercoiled umbilical cords are associated with IUFD, fetal distress, asphyxia, fetal congenital anomalies, and the presence of a single umbilical artery.
The aim of this work is to determine if the umbilical Cord coiling index measurement during second trimester ultrasound scan can predict perinatal outcome. Seventy eight healthy uncomplicated pregnant women who regularly attended the antenatal care clinic for antenatal care and to do anomaly ultrasound scan on her baby in 2nd trimester.
All participants were informed about the aims and the procedures of the study and signed an informed consent form prior to beginning.
Regular antenatal care visit was done every two weeks till delivery with assessment of perinatal outcomes regarding: gestational age at delivery, fetal monitoring by CTG, method of delivery, meconium staining amniotic fluid or not, examination by apgar score at 1stand 5th minute, birth weight, admission to NICU or not and perinatal death.
According to umbilical cord index, of total 78 pregnant women who completed the study 62 (79.2%) were having normal UC coiling, 10 of cases (12.8%) were having hypocoiling and 6 (7.7%) were having hypercoiling.
Our results showed that hypo- and hyper-coiling were associated with increased incidence of preterm labor (32-36 weeks) “22.2%and 40% respectively” while normo-coiling was associated with lesser incidence “2%”. Both hypocoiling “10%” and hypercoiling “16.7%”groups showed higher incidence of IUGR when compared with the normocoiling group “1.6%”. APGAR score at minute one was significantly lower in the both hypocoiling and hypercoiling groups than the normocoiling group with p- value: 0.005. While at minute five, there was no significant difference between the three groups of the study.
Conclusion: The abnormal umbilical coiling index “< 10th percentile or > 90th percentile” is associated with adverse perinatal outcomes. Therefore, early evaluation on Umbilical cord Index in the 2nd trimester can identify fetuses who are at risk and thus help in further management.
The umbilical cord is vital for development, wellbeing and survival of the fetus and it is vulnerable to kinking, compression, traction and torsion, which may affect the perinatal outcome [1].
Vessels of the umbilical cord have a spiral course (pass along the length of the cord in helical fashion). This is called "coiling"of the umbilical cord, which changes as pregnancy advances [2].
A coil is defined as a completed 360 spiral course of umbilical vessel around warton jelly. The umbilical cord coils by the umbilical cord in length in centimeter and called "index of twist" [3].
As measurement of the total length of the cord is not feasible prior to birth, Strong et al simplified calculation of the cord coiling and named it"the umbilical cord coiling index"(UCI). It is calculated as the reciprocal of the length of one complete coiling in centimeters measured antenatally by ultrasound [4].
Abnormal cord coiling index include both hypocoiled cord (cord with abnormal cord coiling index which is below 10th percentile) and hypercoiled cords “cord with an umbilical cord coiling index which is more than90th percentile” [5].
The cause, role and mechanism of umbilical cord coiling have not been elucidated; nonetheless, it has been shown that hypocoiled or hypercoiling of the umbilical cord during 2nd trimester is associated with adverse perinatal outcome such as intra uterine fetal death, intrauterine growth restriction, pre-term labor and fetal distress during labor; consequently, with increased delivery of a low-birth-weight fetus and admission to the neonatal intensive care unit [6].
The aim of this work is to determine if the umbilical Cord coiling index measurement during second trimester ultrasound scan can predict perinatal outcome.
I. Technical Design
This study was Cross-sectional study carried out at Antenatal Care Clinic in Obstetrics and Gynecology Department, Tanta University Hospital. Seventy-eight healthy uncomplicated pregnant women who regularly attended the antenatal care clinic for antenatal care. at the period from January 2019 to January 2020.
Before the start of the study, permission was obtained from the Institutional Review Board “IRB” and Ethical Committee in the faculty of medicine, Tanta University. Also Informed consent from participants included in the study was obtained.
Inclusion Criteria:
Before the start, Approval for this study will be received from the Ethics Committee of the University Tanta Faculty of Medicine, Moreover, written informed consent was obtained from the patients who participated in the study.
Inclusion criteria
The participants in this study were selected according to the following criteria:
EXCLUSION CRITERIA
All patients had history of any of the following were excluded:
II. Operational Design:
Methods
The selected participants will be subjected to the followings:
III. Clinical Examination:
Including Full General and Abdominal Examination
IV.Laboratory Investigations:
Thefollowing laboratory investigations for all participants in the study (done at the Ain shams university Hospitals Laboratories):
Ultrasonographic examination at 22 – 26 GA was done by one investigator using AB 2-7 convex abdominal probe on Voluson 730 Pro Machine (Ge Healthcare, Austria).
Examination will include:
The distance, in centimeter, between two adjacent coils of umbilical artery will be measured from the right outer surface of vascular wall to the right outer surface of its next twist. The coiling index is defined as the reciprocal of the measured distance.
Cases whose umbilical cord coiling index is lower than 10th percentile (<0>Hypocoiled cord, cases whose index is between 10th & 90th percentile (0.1-0.3 coils/cm) are defined as having Normocoiled cords & cases whose index is more than 90th percentile (0.3 coils/cm) are defined as having Hypercoiled cords (according to Strong et al.,1994). (7)
Frequency of follow up visit will be every 2 weeks till delivery.
V.Assessment Of Pregnancy Outcome:
Study design:
This study will be approved from Tanta University Institutional Review Board (IRB).
VI.Statistical Analysis
All statistical calculation were done using computer program SPSS (statistical package for social science; SPSS Inc., Chicago, IL, USA) version 15 for Microsoft Windows.
The percentage of patients who completed the study were 88.6% (78/88), while only 11.4% were withdrawn (10/88) from the study. Of these 10 cases, 4 were excluded because of preeclampsia, 2 were excluded because gestational DM,1 was excluded because of traffic accident, and the 3 cases were excluded because they didn’t attend the antenatal care.
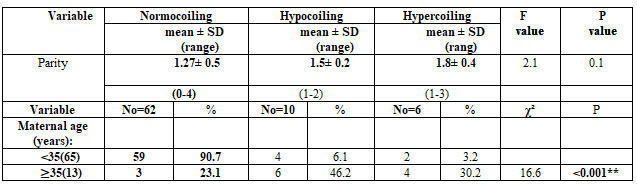
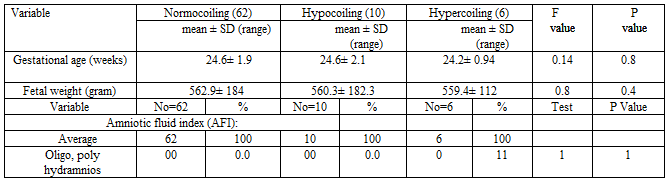
The 78 cases that had completed the study were classified according to the UCI by using ultrasound (at gestational age 22: 26weeks) into; 79.2% (62/78) were diagnosed to be normocoiling, 12.8% (10/78) were diagnosed as hypocoiling, and the rest 6 cases in percentage of 7.7% were diagnosed as hypercoiling. There was not a statistically significant difference between the three groups of the study as regard parity. On the other hand, the majority of the normocoiling group patients were <35>p-value: <0>. There is no statistically significant difference between the three groups of the study as regard gestational age, fetal weight at time of examination (22: 26 weeks) and Amniotic fluid index.
There is no statistically significant difference between the three group
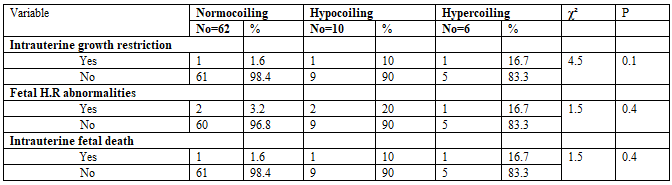
groups of the study as regard IUFD, IUGR and fetal heart rate abnormalities (fetal distress) during antenatal follow up visit.
One IUFD in each of three group occurred during follow up and those patients were excluded from the following tables.
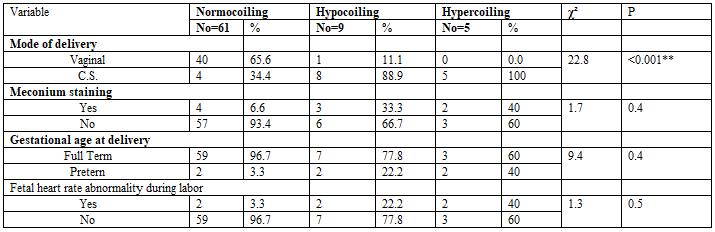
There was a high statistically significant difference between the three groups of the study as regard mode of delivery showing higher rates of Cesarean section in hypocoiling and hypercoiling groups than in the normocoiling group with p-value: <0>.There is also a statistically significant difference between the 3 groups as regard gestational age at delivery with p-value: 0.009.
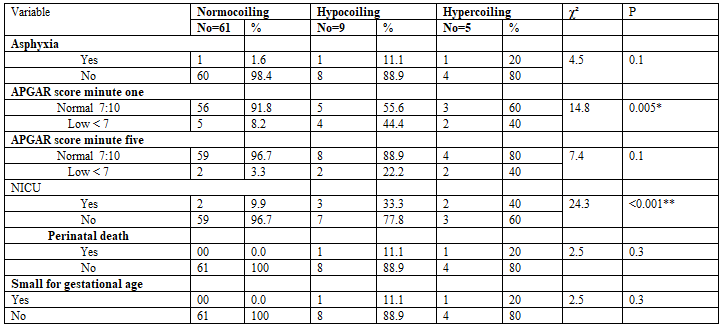
As regard the perinatal outcomes of the three groups of the study, there was a statistical significant difference between them as regard.
APGAR score minute one with p-value: 0.005 with higher rate in the hypocoiling and hypercoiling groups. Also, there was a high statistical significant difference between the studied groups as regard need for Neonatal ICU admission with p-value: <0>with higher rate in the hypocoiling and hypercoiling groups.
The umbilical cord is a very important structure connecting the placenta and the fetus. It consists of 3 blood vessels, and it has the characteristic of screw-shaped coils. The cause, role and mechanism of umbilical cord coiling have not been elucidated; nonetheless it has been shown that the coiling level is associated with adverse perinatal outcome such as intrauterine fetal death, intrauterine growth restriction and fetal distress during labor [8].
Many studies have been carried out evaluating the relationship between UCI and various maternal and fetal outcomes though majority of them have been based on the postnatal UCI. Both hypocoiling and hypercoiling have been linked to various adverse perinatal outcomes [8].
In the light of these studies and keeping in mind the need for further evaluation of the credibility of the antenatal umbilical coiling index, this study was planned to assess the role of the antenatal umbilical coiling as a predictor of adverse perinatal outcome.
According to umbilical cord index, our results showed that of the 78 pregnant women participating in this study, 62 women “79.5%” showed normocoiling, 10 women “12.8%”showed hypocoiling, while 6 women “7.7%” showed hypercoiling.
These results were in agree with that of Patil et al., (2019) who reported in there study on 200 pregnant women that 156 cords “78%” showed normal coiling, 23 “11.5%” showed hypocoiling, and 21 “10.5%” showed hypercoiling [9].
Mittal et al., (2015) found similar results on their study on 200 pregnant women with uncomplicated, singleton pregnancy. They found hypocoiled -UCI <10th>9%);normocoiled- with UCI between 10th –90th percentile (81%) andhypercoiled- UCI >90th percentile (10%) [10].
Also, the study of Adesina et al., (2017) onthe umbilical cords of 436 neonates showed that Normal UCI was observed in 351 (80.5%) neonates, 44 (10.4%) and 41 (9.1%) neonates had hypo- and hypercoiled cords, respectively [11].
The participating women in our study were divided according to the UCI into three groups: normocoiling, hypocoiling, and hypercoiling groups. And further statistical analysis was done on these three groups andour results showed.
As regard maternal age, our results showed that maternal age in normocoiling group was lower than in the other two groups with significant difference between them “p-value: 0.002”as shown in table (2).And when compared between the three groups as regard age < or > 35old we found also a statistical significant difference with p-value <0>indicating that abnormal umbilical cord coiling was common in women > 35 ys.
In harmony with our results was Chitra et al., (2012) as they reported that they found in their study on one thousand antenatal women an association between elderly gravida (>35 years) and both hypocoiled andhypercoiled (P = 0.041 and P = 0.003, resp.) [12].
While Adesina et al., (2017) was against our results and reported that there was there was no statistically significant difference when maternal age, parity and gestational age were compared in the hypocoiled, normocoiled and hypercoiled groups [11].
As regard parity, our results showed that there was no statistically significant difference between the groups of the study with p-value: 0.1.
These results go in harmony with Adesina et al., (2017) as they reported no statistically significant difference when compared parity in their three groups of the study [11].
Also, Patil et al., (2019) reported that on comparing UCI with parity, it was found that there was no statistical significance between primigravida and multigravida [9].
As regard gestational age, at first visit our results showed no significant difference between all groups of the study with p-value: 0.8.
But when we measured the effect of UC coiling abnormalities, our results showed that hypo- and hyper-coiling were associated with increased incidence of preterm labor “22.2% and 40% respectively” while normo- coiling was associated with lesser incidence “2%”.
These results go in agree Jo et al., (2018) who reported on their retrospective study of 251 pregnancies in which a fetal anatomic survey with a recorded UCI was performed at 22-28 weeks gestation that there wasno significant difference between the three groups of their study as regard gestational age at first evaluation. And as regard preterm delivery bothhypocoiling and hypercoiling groups shows higher incidence of preterm delivery “36.4% and 16.7% respectively” than the normocoiling group “7.7% with (p=0.041) [8].
Against these results was Ohno et al., (2016) who reported on their retrospective study, 200 consecutive umbilical cords, that there was no significant difference between the three groups of the study as regard gestational age at birth and incidence of preterm labor [13].
As regard fetal birth weight, at first visit our results showed no significant difference between the three groups of the study with p-value:
0.4. Revaluation of fetal birth weight at delivery time showed also no significant difference between the three groups of the study with p-value:
0.09 despite that both hypo and hypercoiling groups were associated with lower birth weight than the normocoiling guop.
These results go in harmony with Mittal et al., (2015) who reported that Out of the 200 newborn babies, 12 weighed less than 2,500 gm,i.e., were low birth weight babies. Three babies out of these belonged to the hypocoiled group and four belonged to the hypercoiled group. Both hypo- and hypercoiling were found to be significantly associated with low birth weight with p-value “0.0344 between hypocoiling group and normocoiling group and p-value: 0.0095 between hypercoiling and the normocoiling group”. This may well be explained by the increased number of preterm deliveries in the hypocoiled group and a higher number of small for gestational age babies in the hypercoiled group.
While, Jo et al., (2019) found a significant difference between the three groups of the study as regard the incidence of neonates with low birth weights and the incidence in the hypocoiled and hypercoiling groups was 36.4% and 20% respectively, which was significantly greater than the normocoiled groups “10%” with (p=0.044) [8].
However, Kashanian et al. (2016) and de Laat et al. (2017) noted overcoiling and low weight at birth to be significantly related. [14, 15]
As regard the amniotic fluid index, our results showed that there wasno significant difference between the three groups of the study with “p-value: 1.0”.
The results of Jo et al., (2018) showed also no significant difference between their three groups as regard amniotic fluid index [8].
We studied the effect of umbilical cord coiling index abnormalities on fetal outcomes, and we found the following results.
As regard intrauterine growth restriction “IUGR”, our results showed no statistically significant difference between the three groups of thestudy with p-value: 0.1. Both hypocoiling and hypercoiling groups showed higher incidence of IUGR when compared with the normocoiling group with percentage of 10% and 16.7% vs 1.6% [8].
Similar to our results were in agree with Joet al., (2018) who found also no significant difference between their study groups as regard incidence of IUGR in both hypocoiling and hypercoiling group vs the normocoiling group “20% and 25% vs 9.3%” [8].
Against our results was Dakshayini and Meghna, (2020) who found a significant difference between their three groups “p: 0.003”. The higher incidence of IUGR was found in their study in hypercoiling and normocoiling groups “73.3% and 49.3%” while it was lowest in the hypocoiling group “8.3%” [16].
Also, Patil et al., (2019) was against our results as they found a statistically significant difference between their groups “p: <0>
Also, our results showed no significant difference as regard intrauterine fetal death “IUFD” with similar distribution to that in IUGR with p-value: 0.4.
As regard abnormalities of fetal HR, our results showed no significant difference between the three studied groups neither during pregnancy nor during labor with p-value: 0.4 and0.5 respectively.
As regard mode of delivery, our results show a significant difference between the groups with p-value: <0>
These results were in agree with Patil et al., (2019) who found alsoa significant difference between the three groups of the study “p- value: 0.08” with higher incidence of CS in both hypo and hyper-coiling groups while the normo-coiling group showed higher incidence of vaginal delivery [9].
As regard meconium staining of then amniotic fluid, our results showed no significant difference between the three groups of the study with p-value: 0.4. However, this non-significant difference both hypo- and hyper- coiling groups showed higher incidence of meconium staining the normo-coiling group “33.3% and 40% Vs 6.6%”.
Similar to these results Mittal et al., (2015) found no significant difference between hypocoiling, hypercoiling and normocoiling groups as regard meconium staining of amniotic fluidwith p-value “1.000 and 0.300 respectively” [10].
Also, Predanic et al., (2017) found that meconium staining of amniotic fluid was observed more frequently in the group of hypo- and hyper-coiled cords (25.8% [8/31 fetuses] and 22.2% [6/27 fetuses], respectively) rather that in the normocoiled group of subjects (13.1% [31/236 fetuses]). This, however, was not statistically significant (P =
.212, chi-squared test; degrees of freedom, 3.107, 2) [17].
As regard fetal asphyxia, our results showed no significant difference between the three studied groups with p-value: 0.1.
De Laat et al. (2016 a and b) found hypercoiled to be significantly associated with birth asphyxia-acute and chronic [18].
As regard APGAR score, at minute one our results showed that there was a significant statistical association “p-value: 0.005” between the three group of our study with higher incidence of low scores with hypocoiling and hypercoiling groups “44.4% and 40% vs 8.2% in normocoiling group”. While at 5 min, our results showed no significant association “p-value: 0.1” between the three group of our study with higher incidence of low scores with hypocoiling and hypercoiling groups “11.1% and 20% vs 3.3% in normocoiling group”.
Devaru and Thusoo, (2018) found a similar significant association as regard APGAR score at 1 min with p-value: <0>
The result of Mittal et al., (2015) was against our result at APGAR score at 1 min as he found no significant association between their study groups but was agree with ours as regard APGAR score at 5 min with no significant association was found and reported in general that there was no association between poor APGAR scores and umbilical cord coiling abnormalities [10].
Jo et al., (2018) was also against our results as regard APGAR score at 1 min as they found no significant association between their study groups [8].
Adesina et al., (2017) was agree with our results as regard APGAR at 5 min as they found no significant association between their study groups with p-value: 0.201 [11].
As regard the need for neonatal ICU admission, our results showed significant association between the three studied groups with value: <0>
Our results were in agree with Patil et al., (2019) as they found a significant association in the hypocoiling and hypercoiling groups and NICUadmission when compared with the normocoiling group with p- value: <0>
Against our result was Mittal et al., (2015) who found no significant association between their both hypocoiling and hypercoiling groups vs the normocoiling group as regard NICU admission with p- value: 1.000. in this study no NICU admission was recorded in the hypocoiling and hypercoiling groups while 3 cases were recorded in the
nornociling group [15].
Also, Adesina et al., (2017) found no significant difference between was observed in their study as regard NICU admission with p- value: 0.976 [11].
The abnormal umbilical coiling index “< 10th percentile or > 90th percentile” is associated with adverse perinatal outcomes. Therefore, early evaluation on Umbilical cord Index in the 2nd trimester can identify fetuses who are at risk and thus help in further management.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
